10 fun facts about orthodontics
What are the most interesting facts about this dental speciality we need to know?
As dental professionals, we provide orthodontic treatment to our patients, whose chief concern is usually the appearance of their misaligned teeth. The appearance of the upper or lower front teeth usually brings the prospective patient to our clinic for a consultation.
Nowadays, various orthodontic appliance types can improve the position of crooked teeth. Removable clear aligners have been used successfully for a decent amount of time. However, fixed braces are still the gold standard in orthodontics. I truly believe these aesthetic removable appliances are the future of orthodontics and dentofacial orthopaedics.
However, some types of tooth movements are still challenging for them. For example, complex rotations and extrusion are still problematic for aligners. However, the attachments, the plastic used, and the forces applied to the dentition are constantly improving – but we definitely need more time.

Regardless of the manufacturer, most cases can be treated to a predictable end result with aligners. If we as dentists are familiar with the basics in the biology of tooth movement biomechanics and can critically assess the treatment suggested to us in the simulation. Accepting the technician’s treatment option without critically assessing it will probably lead to an unpredictable end result and a difficult conversation with the patient.

The dental profession has benefited tremendously because aligning the teeth before initiating restorative procedures expands patients’ and dentists’ available treatment options. For example, orthodontics can significantly improve the periodontal condition in specific clinical scenarios. Orthodontists prefer to have the adjacent teeth and their roots reasonably aligned before implant placement is considered and performed.
Let us not forget that straight teeth and a beautiful smile are usually the main requirements of the patient. However, we need to obtain a stable static and dynamic occlusion at the end of the orthodontic treatment that will serve our patients well for the rest of their life. That’s why choosing the appropriate appliance for the specific clinical case is the responsibility of the clinician, not the patient.
The vast majority of adult patients seek removable clear aligners, but in my opinion, as an orthodontist, they are not a perfect fit for every case.
Orthodontics – more than treatment for your patients
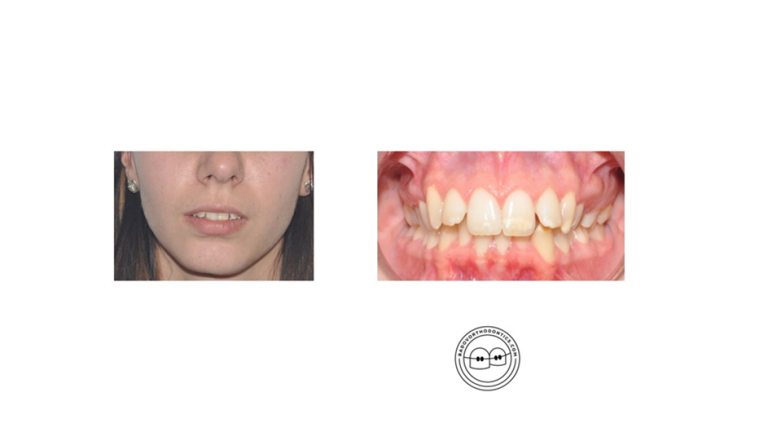
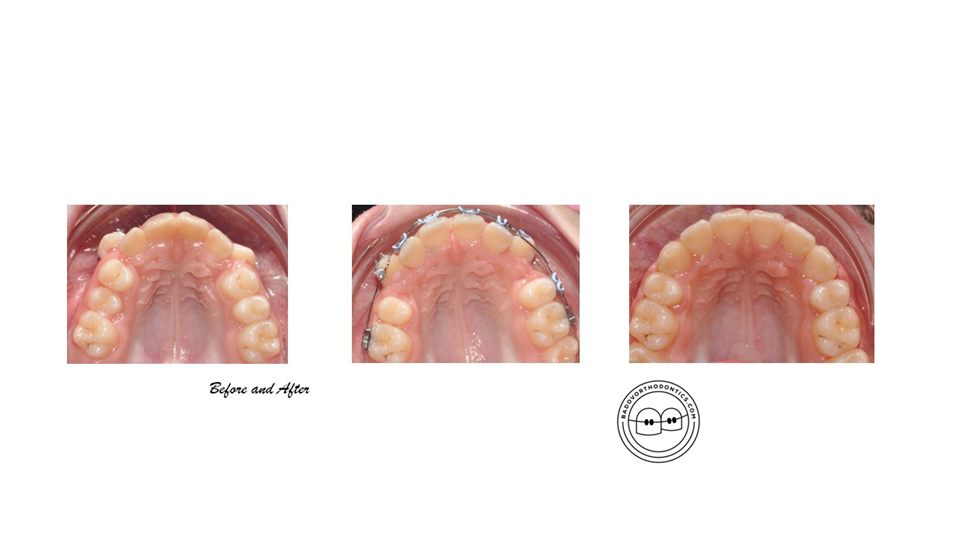
Some people believe that the appearance of their teeth can significantly improve their self–esteem, career opportunities, etc. I think we clinicians should not give unrealistic expectations to our patients. I personally show the beginning and end photos of cases with similar malocclusions that I have treated and explain what I can offer as a clinician.
During the initial clinical exam, I try to understand what bothers the person sitting in front of me. Is it the abnormal positioning of the teeth that is the chief concern, or does the treatment plan have to address both the appearance of teeth and jaws?
One of the main goals of treatment is moving teeth into their ideal and desired position. For example, we can significantly improve the soft tissue profile after successfully correcting an increased overjet. Improving the soft tissue profile is more important than obtaining a good-looking occlusion on orthodontic study models. We all, as clinicians, can agree on that without hesitation.

Sometimes, the appearance of the face and profile can only be achieved with the help of combined orthodontic and surgical treatment. After the age of 18, aligning jaws can happen only after orthognathic surgery. With that valuable treatment option, we can address not only severe skeletal discrepancies in all three dimensions but also facial asymmetries.
Many patients do not know much about that option. If I believe that the case can be treated with that combined approach, I will encourage the patient to meet the maxillo-facial surgeon that I work with. I am not pushing the person, and I do not insist on him or her getting his or her jaws broken. I just want the patient to gather all of the information so he or she can make an informed decision.
So, it is that kind of improvement you can offer your patients that can really change their appearance. Of course, suppose you do not feel confident offering those treatment modalities as a dentist. In that case, you can just write a referral for a consultation with a multidisciplinary team in your area. Your patient will definitely appreciate that.
Ten interesting facts about orthodontics
Here are some interesting facts about orthodontics.
1. The Father of Orthodontic Speciality
We all know from dental school that Edward Angle is considered the father of orthodontic
speciality. It is fascinating for clinicians to learn more about his treatment philosophy and approaches. He was absolutely against extractions of teeth. Braces back then did not actually exist.
The first orthodontists literally tied the crude metal bands wrapped around the teeth with metal alloys. Precious metals like gold were sometimes used because modern archwires and their properties were unavailable.
2. Who introduced the extractions of teeth
It was Angel’s students who introduced the extraction of teeth as a valuable treatment option
for crowded teeth. Problems like severe proclination of the incisors and relapse were some of their chief concerns as clinicians.
3. The standard of oral hygiene
Your patients’ standard of oral hygiene will reveal their determination for treatment. Before we begin orthodontic treatment, the patient must present with healthy gums, no tooth decay, and no other sort of mouth pathology.
Every dentist knows that maintaining a high standard of oral hygiene can be quite challenging for some patients, especially teenagers.
Patients who do not follow the orthodontist’s instructions will most probably have a problem cooperating with the clinician throughout the course of treatment. The end result will be white spot lesions, gum disease, and caries, and in some cases, the treatment will have to be terminated before an adequate end result can be achieved.

4. Every orthodontic appliance can straighten teeth
It is a scientific fact that if we apply light and continuous gentle pressure for more than 6 hours a day, teeth will move in the desired direction. They do not know if they are wrapped around plastic aligners or if fixed appliances are being bonded. What we actually do is either push or pull the teeth and by doing so, we cause bone remodelling.
Bone apposition and resorption occur simultaneously during dental movement. We, as clinicians, are in total control of the movement, and we need to avoid damaging pressure on the periodontal ligament that occurs when heavy forces are applied to the teeth.
5. Malocclusions
We can successfully treat mild and moderate Class II and Class III malocclusions by providing the so-called camouflage treatment.
Let’s consider for a second a Class II div 1 malocclusion that needs to be corrected. The reasons for this skeletal discrepancy could be that the upper jaw is prominent (prognathic), the lower jaw is in a distal position (retrognathic), or a combination of both. The increased overjet could also be due to prominent upper teeth.
That is a brief explanation of the sagittal discrepancy. Of course, we need to consider possible transverse and vertical deviations from the norm. The presence of an increased overjet could be combined with an anterior open bite and tongue thrusting habit as well.
Orthodontic treatment options for these malocclusions include the initiation of teeth extractions before tooth movement. The space provided by the missing teeth is utilised to correct crowding and obtain normal incisor relations in terms of overjet and overbite.
We usually extract upper premolars in Class II cases and lower premolars or lower incisors in Class III cases. Sometimes, extractions in both arches have to be performed.
6. Growth modification for some Class II cases can be extremely successful
Both functional appliances and extraoral appliances like headgear are useful orthodontic instruments for the treatment of growing patients who need orthopaedic correction. From the available literature, we know that that is a valuable treatment option, and in some cases, it can avoid the need for an orthognathic surgery of the lower jaw.
The growth potential of the patient, cooperation, and timing of the treatment are the most important factors determining the outcome.
7. Removable retainers are probably the most widely used retainers nowadays.
Vacuum-formed retainers and Hawley retainers are probably the type of retainers that every patient receives at the end of treatment. Fixed retainers are also widely used, but their main disadvantage is that they can be debonded from a tooth or even broken without the patient noticing it.
With time, it will cause a relapse in the position of the teeth and frustration for the patient. This is probably the main reason why most experienced clinicians always provide a removable retainer on top of the fixed one. Two is one, and one is none.
8. Most teenagers do not realise that braces are different from jewellery
By bonding braces to teeth, we provide dental care by resolving the crowding in the arches and improving the bite. However, most teens do not see it that way. For them, it is a fashion trend and something like jewellery, and most of them do not mind wearing classical braces. I have been asked if metal detectors at airports can alert security because of their braces.
9. Crowding of teeth and their proclination is a different visualisation of the same problem
The position of the teeth depends on the actual space in the arch and the soft tissues around the teeth. The periodontal ligament, the lips, cheeks, and tongue determine the position of the dentition. It is common to examine a patient with aligned arches, incomplete overbite, and significant proclination of upper and lower teeth.
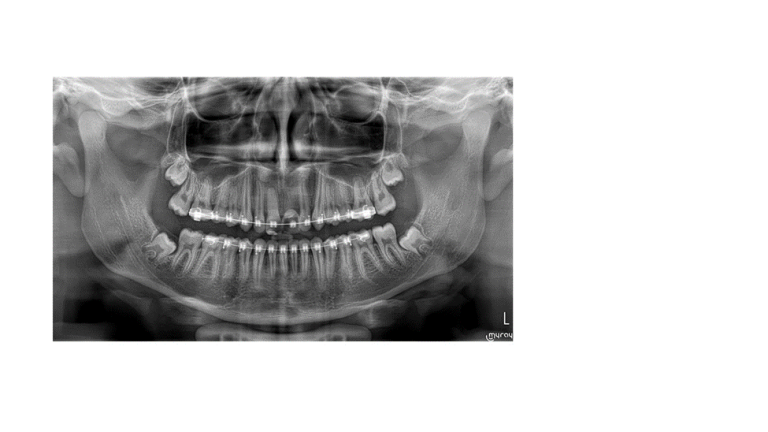
After the cephalometric X-rays have been analysed, an accurate assessment of the proclination is possible. However, extraoral clinical signs like incompetent and prominent lips at rest can lead us to this assumption.
10. Cases that present with mild and moderate crowding can be treated by both extraction or non-extraction
Different clinicians approach the same case in totally different ways. It really comes down to the dentist’s experience, appliance of choice, and training. Extractions are seldom performed in cases with mild crowding. Most of us will utilize proclination, expansion of arches, and IPR to get the job done.
However, moderate crowding is often resolved after extractions. Some clinicians feel comfortable resolving around 7-8 mm with IPR, while others will consider extractions of premolars or a single lower incisor. There are no written rules about it, and every clinician can justify his or her approach to treatment.